Docobo Ltd - Glasgow City Region
Enhancing Rural Patient Monitoring with 5G in Inverclyde, I-FIVE uses 5G connectivity to enhance rural monitoring and video consultations for patients with long-term conditions at home and in care homes across Inverclyde, Glasgow City Region.
Funded by the Department of Science Innovation and Technology (DSIT) as part of the 5GIR programme, Glasgow City Region (GCR) utilised circa £750,000 to develop an innovation scheme, ensuring rapid outcomes within an 8-month period across the 5G Glasgow City Region (GCR) between September 2004 and March 2025. As part of the Smart and Connected Social Places Program, the Docobo innovation project, I-FIVE aims to demonstrates how 5G connectivity can improve rural patient monitoring for individuals with chronic conditions in Inverclyde.
Building on a decade of successful telehealth delivery, the project introduced enhanced video-enabled monitoring for 20 community-based COPD patients and two local care homes supporting up to 120 residents. In the I-FIVE Project, Docobo Ltd (a wholly owned subsidiary of Graphnet Health) In partnership with Inverclyde HSCP, tested the impact of 5G-enabled tablets and remote care pathways to extend access, reduce avoidable hospital admissions, and improve care outcomes in both community and residential care home settings.
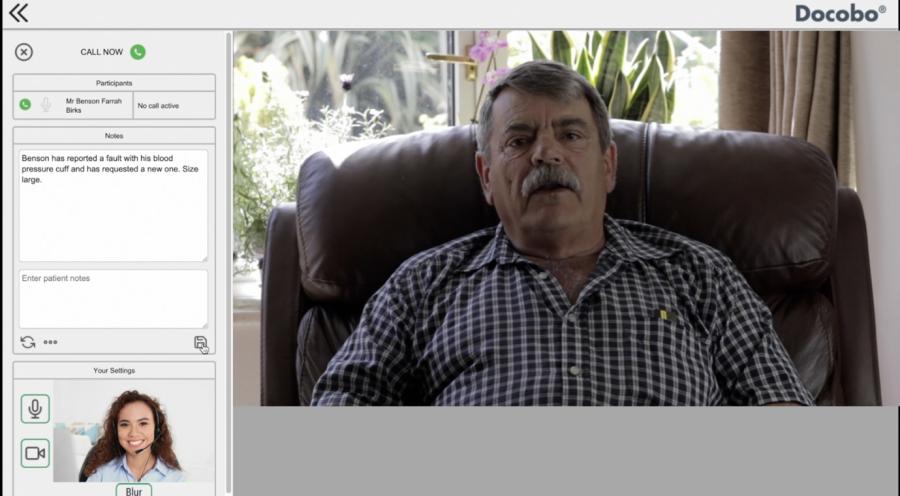
The pictures below show patients using the devices in both Community and Care Home settings.



Community based COPD Patient using the 5G enabled Tablet Device in Video Call

Care Home Patient being assisted by Care Staff to capture the Patient Data
What is the Problem to be solved?
Who is the case study aimed at?
This case study is intended for NHS leaders, local authorities, care home operators, and digital transformation professionals across health and social care. It is particularly relevant to decision-makers aiming to reduce health inequalities and address long-term condition management in rural and deprived areas.
Description of the problem or challenge:
Inverclyde faces some of the highest levels of deprivation in Scotland, with life expectancy and health outcomes significantly below the national average. One in four residents is aged over 65, with this figure expected to rise by 38% by 2050. Chronic conditions such as COPD, diabetes, and heart failure are disproportionately prevalent, placing immense pressure on overstretched services. Meanwhile, traditional care pathways struggle with delayed access to GPs, A&E, and hospital-based support.
Care homes in the region had no previous remote monitoring infrastructure in place. In the community, existing telehealth services relied on dated PSTN infrastructure or broadband Wi-Fi, which limited access to high-quality video consultations, particularly for digitally excluded or low-income households.
Barriers to development or adoption:
- Inconsistent broadband and limited 5G penetration in some areas
- Building infrastructure obstructing in-building 5G signal
- Limited digital skills and confidence among staff and patients
- Technical integration with NHS clinical systems
- Short pilot duration limiting full outcome measurement
Who are the sector operators and suppliers involved?
- Docobo Ltd: Supplier of the DOC@HOME platform, patient app, hardware, and implementation support
- Inverclyde Health and Social Care Partnership (HSCP): Clinical delivery and care pathway coordination
- Vodafone: 5G connectivity provider, supporting technical enhancements such as antenna reconfiguration
The I-FIVE project was designed to address these issues by trialling high-speed 5G-supported remote patient monitoring and video consultations in the homes of 20 COPD patients and across two residential care homes supporting up to 120 residents with complex health needs.

Care Home Patient being assisted by Care Staff to capture the Patient Data using the DocoboApp
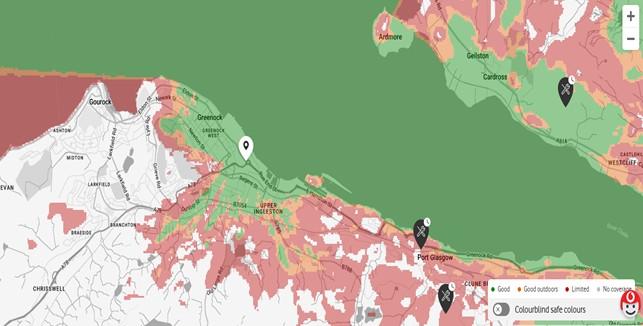
Vodafone 5G Coverage Map for Care Homes Located in Greenock West
What is the solution to the problem?
The I-FIVE project deployed 5G-enabled remote monitoring using Docobo’s DOC@HOME platform and patient-facing DocoboAPP, installed on the 5G Tablet Device combined with medical-grade peripheral devices (blood pressure, SPO2, temperature monitors). The solution allowed both community patients and care home residents to submit vital signs and symptomatic data, triggering clinician review and enabling video consultations in response to alerts.
Detailed technical solution:
- Community COPD patients were issued 5G-enabled tablets preloaded with DOC@HOME and a structured COPD question set.
- Patients submitted daily data from home to the DOC@HOME platform via the 5G Network which was triaged at the Clinicians Portal.
- Video consultations were initiated by the care team when alerts were triggered or for routine wellbeing checks.
- In care homes, staff used multi-resident tablets to input data and complete assessments using tools like RESTORE2.
- Clinical teams accessed submitted data in real time and could initiate video consultations with staff and patients directly.
- A Patient Clinician Workflow example is shown below.
Implementation and deployment:
- 20 COPD patients received 5G tablet kits for home use.
- Two care homes (Little Sisters of the Poor and Alt-Na-Craig House) received four shared-use tablets, supporting approximately 120 residents.
- Cellular modems were installed to mitigate weak indoor 5G signals caused by stone buildings and concrete infrastructure.
- Clinical staff were trained in use of the platform, video calling, and interpreting patient-reported data.
Suppliers involved:
- Docobo Ltd: remote monitoring platform, app development, and medical hardware.
- Vodafone: 5G infrastructure and network engineering (e.g. antenna down-tilt for coverage improvement).
- Inverclyde HSCP: frontline delivery, training, and clinical triage.
Connectivity requirements:
- Video consultations and high-bandwidth data transfers required a stable 5G connection, ideally at speeds of 10 Mbps or higher.
- In areas where 5G penetration was low, Vodafone installed Gigacube cellular modems or adjusted antenna configurations to ensure signal quality.
- Where buildings presented signal attenuation challenges (e.g. Faraday cage effect), signal boosters and powerline Wi-Fi extenders were trialled.
Network options and considerations:
- 5G offered reliable and fast communication for video consultations without requiring home broadband—especially beneficial in low-income areas.
- In-building Wi-Fi generated from 5G cellular modems helped increase compatibility with existing devices in care homes.
- PSTN and 4G were used as fallback options in locations where 5G coverage remained poor.
Key enablers:
- 5G-enabled Android tablets (DocoboAPP preloaded)
- Medical-grade vital signs monitors (BP, SPO2, thermometer)
- Secure cloud infrastructure (data presented to clinicians via portal)
- RESTORE2 and NEWS2 scoring integration in care homes
Energy consumption:
- The devices used were low-power tablets designed for continuous monitoring and were supported with regular charging infrastructure.
- Cellular modems added minimal energy load and were installed in accessible locations.
Safety considerations:
- DOC@HOME is a medical device regulated under CE marking.
- All clinical data is encrypted and stored securely.
- The system includes escalation protocols for clinical review in the event of alerts or deteriorations.
Product integration:
- Plans are in place for future integration with NHS systems such as TrakCare and EMIS to improve data flow across care settings.
- RESTORE2 scoring is embedded in the platform to support ambulance service referrals.
Patient Clinician Workflow Example

- Patient enters Blood Pressure Data using the DocoboApp on the 5G Tablet Device and it is transmitted to the DOC@HOME Platform via the 5G Network
Clinician views the Patient Data using the DOC@HOME Clinicians Portal
Image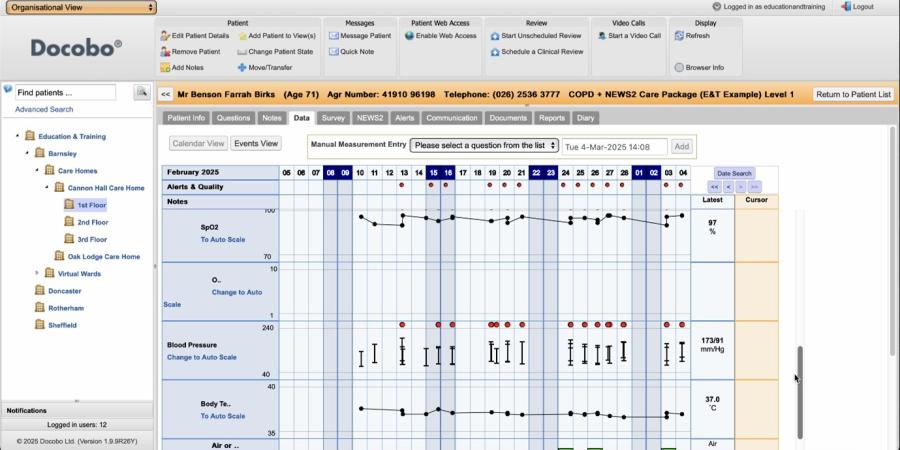
- Clinician Triages Patient Data and Alerts displayed on the Clinicians Portal
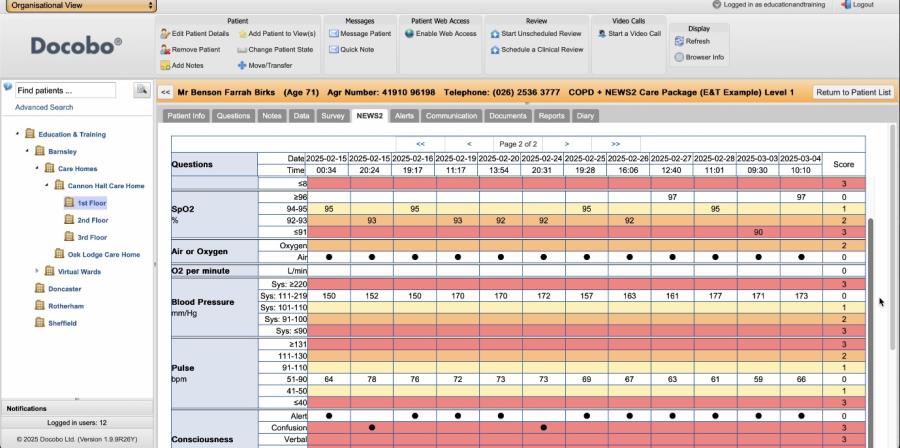
- Clinician generates NEWS2 Score on the Clinicians Portal from the Patient Data if required
5. Clinician makes a secure Video Call Directly to the Patient via the DocoboApp in response to the NEWS2 Score and alerts and determines if an intervention is required
Commercial model (Business Case)
The I-FIVE project offers a scalable, cost-effective model for digital healthcare delivery using 5G-enabled remote patient monitoring. It provides both short-term efficiencies and long-term savings by reducing avoidable hospital admissions, emergency callouts, and routine GP visits.
Benefits
The I-FIVE project has demonstrated a wide range of benefits for patients, clinicians, care staff, and the broader health and social care system. These include:
Digital inclusion:
- Patients and care homes without prior access to remote monitoring have now been engaged with easy-to-use digital tools.
- Patient Information videos concerning the patient’s condition and Self-Care Advice are delivered through the 5G Tablet, with updates and new content being able to be uploaded more quickly.
Lessons Learnt
Do's
- Do build on trusted partnerships. The long-standing relationship between Docobo and Inverclyde HSCP was vital in delivering the project at pace and ensuring clinical buy-in.
- Do plan for diverse settings. Anticipate the technical challenges of 5G in older buildings and signal-poor areas, use cellular modems or alternative Wi-Fi boosters to extend coverage.
- Do invest in training and digital onboarding. Both care staff and older patients benefitted from structured, supportive training to build confidence in using the technology.
- Do embed tools like RESTORE2 and NEWS2. These enhance clinical decision-making and empower care home staff to escalate issues appropriately and efficiently.
- Do capture patient and carer stories. First-hand feedback added powerful qualitative insights that helped validate impact and strengthen stakeholder support.
- Do collaborate with network providers early. Vodafone’s proactive involvement enabled faster fixes and antenna adjustments to extend coverage.
- Do ensure a multi-phase rollout. Phased implementation allowed time for technical testing, staff training, and live monitoring, with scope to gather feedback before full deployment.
Don’ts:
- Don’t assume all devices are pre-approved. An Android version mismatch on Samsung tablets required rapid re-certification of the Docobo app, causing initial delays.
- Don’t overlook device interaction with enterprise security tools. Knox security integration created unexpected compatibility issues that needed urgent resolution.
- Don’t rely solely on in-building 5G. Many buildings, especially in older communities, are constructed in ways that block signal, plan for Gigacube or Pico-cell solutions where needed.
- Don’t underestimate the variation in adoption speed. Care homes adopted the technology at different rates, tailored support and continuous engagement were essential to build momentum.
- Don’t delay gathering qualitative feedback. Early patient and carer surveys, including PROMs and PREMs, informed real-time refinements and supported the sustainability case.
If you’re ready to embark on a connectivity project, we can point you to the suppliers with expertise in your sector.