The Liverpool 5G network was deployed between September 2020 and September 2022 as part of the DCMS 5G Create programme. At the time, this was the largest 5G Stand Alone network to be deployed in a community setting.
This case study looks at the learnings and how this can be applied in the current context, with practical suggestions for the future adoption of civic networks to provide the infrastructure needed to support the growth of digital public services.
What is the problem to be solved?
The motivation for building the network at the time was as follows:
- Many existing Telecare solutions depended on analogue systems, which were due to be switched off in 2025
- Many households have no access to affordable, reliable connectivity. This impacts on isolation, education, health and social care.
- The digital divide increased exponentially during COVID-19. The impact of Digital Poverty is now widely recognised.
- The Liverpool City Region faces vast, complex health challenges and increasing health inequalities.
- Service Level Agreements to support technology based monitoring solutions in the community are not available or cost prohibitive.
- Increasing amounts of NHS and Local Authority revenue budget were being spent on providing commercial connectivity.
What is the solution to the problem?
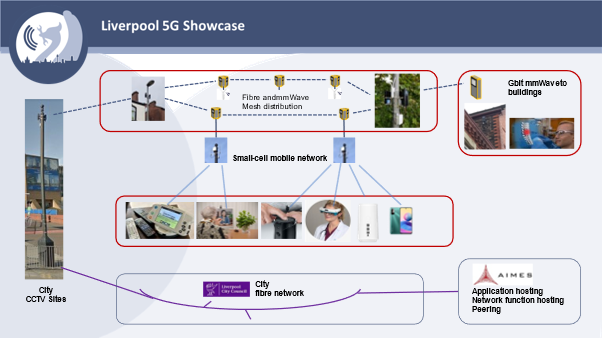
The network brought together the latest 5G small cells and mmWave equipment using existing street furniture, supported by Liverpool City Council. A range of equipment, configured to use the network, was supplied to people’s homes. This meant that services could use the high-capacity network without incurring data charges or limiting data usage, irrespective of the commercial connectivity available in the premises. Our network design was one specific example of how a private 5G Stand Alone network could be deployed. At the time we were the first to be deploying 5G small cells at scale and as early adopters the equipment costs were high, reflecting the R&D environment. The project proved that the technology was available, and that the deployment was feasible.
The network was deployed in the Kensington area of Liverpool. Examples of the applications deployed are as follows:
- Telehealth monitoring – Docobo devices were deployed to people’s homes and care home settings. Although this service can be provided without our network, they were SIM enabled and data usage was capped, meaning that the use of videos on the device was limited. The NHS bore the cost of the SIMs. By providing devices configured to connect to our stand-alone network, there were no data charges incurred and no limits on data usage.
- Education – primary school children could work on Chrome Books in school that were configured to connect to our network when they took them home. This meant children were not disadvantaged if they did not have connectivity at home.
- Care Homes – the standard of connectivity available in care homes varies widely. The impact of this means that remote NHS services cannot be deployed across all care homes. We connected care homes to the network, giving residents access from their rooms and bringing the care homes up to the required standard of connectivity.
- GP Surgeries – we connected GP surgeries in the area, giving improved performance and potential cost savings against the current connectivity model.
- Supported Living – we worked with care providers to provide connectivity to supported living buildings. This enabled staff to access digital services, supported the use of sensors in the property leading to increased security and independence for residents.
More information on the technical solution is available at www.liverpool5g.org.uk
Commercial model (Business Case)
Although the technology solutions were feasible, the creation of a business plan was more challenging. Liverpool City Council, the partner driving the need, was unable to take the project further as although there were benefits, this was not seen as part of their core activity and other priorities were more important at the time. This only supports our conclusion that the use of private networks needs to be considered at a more strategic level, bringing together all the public bodies in the area.
Each of the applications we trialled could go ahead to some degree without a private network. Each application would need a business case of its own to demonstrate the specific costs and benefits for the service. Connectivity could be provided on a commercial basis with revenue costs incurred and capacity limitations.
Not all benefits from the services would be able to be monetised, they may be social, preventative or equate to cost savings within different budgets. For example, reduced medication errors in home care services (social care) leading to reduced hospital admissions (NHS). This treatment of benefits in budget silos acts as a practical barrier to the adoption of technology within services. The potential value creation comes in the form of shared connectivity infrastructure provision through a private network.
On reflection, the work conducted on the business model during the project had the wrong focus. The focus was on specific services, but it should have been on providing the connectivity infrastructure to support all digital services across all public bodies in the region.
The project proved that the proposed technology approach was feasible. As time has moved on there is more equipment available on the market and prices have come down, further supporting the technical feasibility and the business case.
Benefits
Benefits evidenced from the specific trials conducted under our projects include:
- Potential cost savings to the health and social care services of ~ £2,477 per user per year
- Reduced cost of connectivity to NHS
- Released more than 300 carer hours per user per year
- Medication costs reduced by over 50%, and medication wastage reduced.
- Decrease in medication errors: 51% drop in the number of service users who had a medication error
- Reduced cost of health services to treat cat 4 pressure ulcers
- Improved service for patients – Improved quality video service capability with a better user experience for teleconsultation
- Better health outcomes for residents and reduced costs to NHS due to decreased number of falls and hospitalisations
- 40% increase in service users who felt more independent
- Reduced travel time and costs for patients
The above benefits were demonstrated from specific services that trialled equipment on the network. Providing the network as infrastructure to support a wider range of public services will lead to increased benefits for both residents and services. Detailed L5G project benefit reports 2020 and 2022 are available at www.liverpool5g.org.uk
Lessons Learnt
- The key lessons learnt can be summarised as follows
- Social Care is very different to NHS – this needs to be recognised, resisting the temptation to treat health and care services as one.
- The full stakeholder chain needs to be considered across services for successful adoption. Any link in the chain can block successful adoption if not given meaningful consideration.
- To consider infrastructure decisions across regions need to elevate approach to strategic/regional level – no single public body can make these decisions.
- Budgets – the cost of connectivity is not new money, it already exists in connectivity budgets for the individual services.
- The business model was wrong to focus on connectivity within use cases, it should consider connectivity as infrastructure provision across services and across regions.
- Building on the learning from the Liverpool 5G projects we have now produced a white paper on the case for civic networks. This document can be found here - https://liverpool5g.org.uk/the-case-for-civic-networks-l5g-white-paper/
- The wider use of the civic network model would:
- Lower costs for all public services involved
- Provide better connections, better quality services, efficiencies and improvements across health and social care services, education, housing and transport
- Reduce the digital divide
- Drive regeneration and growth
Meet government vision and priorities
If you’re ready to embark on a connectivity project, we can point you to the suppliers with expertise in your sector.